

Many rehab teams hear about exoskeletons, but few get a clear definition. That gap creates hesitation, mixed expectations, and slow decisions when new gait technology enters the discussion.
A gait training exoskeleton is a powered rehabilitation device that supports and guides lower-limb walking practice under clinical supervision. It is not a simple brace, not a consumer wearable, and not a cure. In rehab, it helps therapists deliver structured gait training with more consistency and less physical strain.

I have spent more than 20 years in medical device export, and I have seen one pattern again and again. A product category grows much faster once buyers share the same basic definition. That is why I see this article as an anchor. If a rehab director, physiotherapist, or distributor technician wants to understand gait exoskeleton rehabilitation in plain language, this is the starting point. I will explain what a gait training exoskeleton is, how it works, where it fits, and where its limits begin.
Definition — What Is a Gait Training Exoskeleton and What Is It Not?
Many people group braces, walkers, and robotic devices into one bucket. That confusion leads to wrong comparisons, wrong budgets, and wrong clinical expectations.
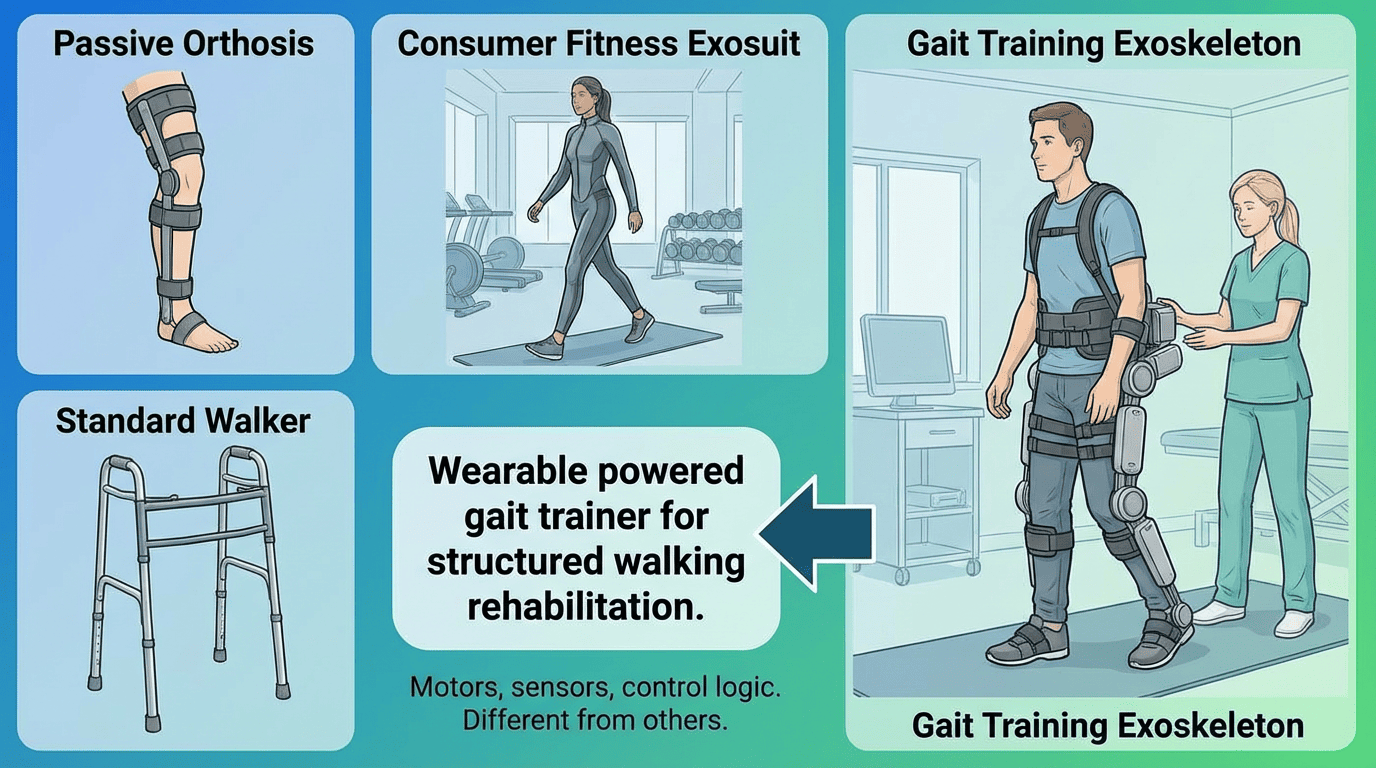
A gait training exoskeleton is a wearable powered gait trainer for structured walking rehabilitation. It uses motors, sensors, and control logic to support lower-limb movement during therapy. It is different from a passive orthosis, a standard walker, or a consumer fitness exosuit.
When I explain this category to hospitals and distributors, I start with one simple point. A gait training exoskeleton is a rehabilitation tool. It sits inside a clinical process. It does not replace clinical judgment.
What the device is
A Gait Training Exoskeleton usually supports the lower limbs and trunk alignment during walking practice. The system uses powered joints, sensor input, and preset or adjustable training modes. The therapist sets the session goals, selects the support level, and monitors the patient throughout training.
Most hospital buyers need to separate this from two other categories:
| Category | Main purpose | Power source | Typical use setting | Key limitation |
|---|---|---|---|---|
| Gait Training Exoskeleton | Structured gait rehabilitation | Powered actuators | Hospital or rehab center | Requires trained supervision |
| Passive brace or AFO | Joint positioning or stability | No motor power | Clinic, hospital, home | Does not drive gait pattern |
| Consumer wearable | Daily mobility or wellness support | Varies | Home or lifestyle setting | Not designed as clinical gait training equipment |
What the device is not
A gait training exoskeleton is not a magic machine. It does not restore walking by itself. Research suggests that robotic gait training can support repetitive task-based therapy, but individual results depend on patient profile and clinical protocol.
It is also not the same as a simple mobility aid. A walker helps a patient move. A powered gait trainer helps a therapist deliver a planned training session.
It is not for unsupervised home use in most clinical discussions. In the settings we work with, the device belongs inside professional rehabilitation workflows.
In a first meeting with a rehabilitation hospital in Europe, the team asked us a question that sounded simple: “Is this basically an AFO with a battery?” One therapist thought the device was a brace. A purchasing manager thought it was closer to a consumer walking aid. The rehab doctor was not sure where it fit at all. Everyone used familiar words, but they were talking about different product categories.
We stopped the pricing discussion and went back to basics. We drew three columns on a whiteboard: brace, consumer mobility device, and rehabilitation exoskeleton. Then we explained the difference in role. A brace mainly supports alignment or positioning. A consumer mobility device helps with daily movement. A rehabilitation exoskeleton supports structured training or supervised walking progression, depending on the type.
That changed the meeting immediately. The therapists started asking clinical questions instead of general product questions. The purchasing manager stopped comparing it with low-cost daily aids. The doctor began discussing which patients were in the transition phase and which ones still needed a full gait trainer.
By the end of the meeting, the hospital team no longer asked, “What is the price of this device?” They asked a much better question: “Which stage of our rehab pathway is missing the right tool?” That was the moment the conversation became productive.
How Does a Gait Training Exoskeleton Work?
Exoskeletons can seem complex from the outside. That complexity often makes clinical teams worry that setup will be difficult or that the machine will control everything.
A gait training exoskeleton works by combining powered actuators, body support, and gait detection logic. The system assists selected phases of walking while the therapist adjusts settings for patient ability and training goals.

The easiest way to understand the system is to break it into parts. Most rehab professionals do not need engineering detail. They need a working model of what each part does during treatment.
Powered actuators
The powered joints create controlled assistance at the hip, and in some systems at the knee. This support helps guide limb movement through a planned walking pattern. The therapist can often adjust assistance level, step parameters, and training mode.
This does not mean the patient becomes passive. In good practice, the team uses assistance as needed, not more than needed. The goal is to support movement quality and session intensity under professional supervision.
Gait cycle detection
The system uses sensors to detect motion state, step timing, and sometimes load or posture changes. The exact method depends on the model. Some systems use joint angle feedback. Some use foot contact or force-related input. Some combine multiple signals.
This sensor layer matters because walking is not one single action. The body moves through phases. A useful exoskeleton needs to recognize those phases well enough to deliver support at the right moment.
Weight support and stability mechanisms
Some gait exoskeleton rehabilitation systems work with walkers, support frames, or harness-based setups. These features help reduce fall risk and make early-stage gait practice more manageable. They also help the therapist spend less effort on pure physical lifting.
What the therapist controls
The therapist still controls patient selection, setup, progression, and stopping rules. The machine provides repeatable assistance. The clinician provides the treatment logic.
| Functional part | What it does | Why it matters clinically |
|---|---|---|
| Actuators | Assist joint movement | Supports step repetition and pattern guidance |
| Sensors | Detect gait timing and movement | Helps the system respond during walking |
| Body support elements | Improve safety and positioning | Makes training possible for weaker patients |
| Software settings | Adjust mode and intensity | Lets the therapist tailor sessions |
Who Uses a Gait Training Exoskeleton in Rehabilitation?
Hospitals often ask one practical question first. Which patient groups actually fit the device, and which do not?
Gait training exoskeletons are used for selected patients with stroke, spinal cord injury, neurological conditions, and some post-surgical rehabilitation needs. Use depends on mobility level, goals, safety criteria, and therapist judgment.

In real clinical work, the answer is never just diagnosis. A device may suit one patient with stroke and not another. The same is true for SCI and post-surgical cases.
Common use cases
Many rehab centers look at this category for:
- Stroke rehabilitation
- Spinal cord injury rehabilitation
- Neurological gait disorders
- Post-surgical gait re-training in selected cases
- Geriatric rehab cases where assisted repetitive gait practice may be appropriate
Research and clinical feedback indicate that these systems can help deliver structured, repeatable training under professional supervision. Individual results depend on patient profile and the therapy plan.
Factors that matter more than diagnosis alone
I always encourage buyers to look at function, not only labels. These questions matter:
- Can the patient tolerate upright training?
- Can the patient follow instructions?
- Does the patient need full, partial, or minimal limb assistance?
- Does the team have the staffing and space to run the sessions safely?
- Does the department want early standing, guided overground practice, or later-stage walking intensity?
Clinical fit overview
| Patient group | Possible use | Key consideration |
|---|---|---|
| Stroke | Repetitive gait practice | Tone, balance, cognition, fatigue |
| SCI | Supported stepping and task practice | Injury level, trunk control, transfer ability |
| Neurological conditions | Guided mobility training | Disease stage and variability |
| Post-surgical rehab | Selected gait re-training cases | Surgical protocol and load limits |
I remember a discussion with a rehab department that began with a long list of diagnosis labels.
The team asked whether the device was for stroke patients, SCI patients, or neurological cases, as if the diagnosis alone would decide everything. We then shifted the conversation to function. We asked simple questions:
Can the patient tolerate standing?
How much trunk control do they have?
Can they follow instructions?
What level of fatigue appears during training?
That changed the tone of the meeting. The therapists started grouping patients by walking potential, support needs, and training goals instead of by diagnosis name alone. A stroke patient with poor balance and high fatigue needed a very different approach from another stroke patient who could already initiate stepping. The same was true for SCI and other neurological cases.
Once the department moved from diagnosis-based thinking to function-based selection, the clinical fit became much clearer.
What Are the Three Main Types of Gait Training Exoskeleton?
Many buyers think all robotic walking systems are basically the same. That assumption can lead to poor product fit and unrealistic demos.
The three main types are overground exoskeletons, treadmill-based systems, and hybrid configurations. Each type supports gait rehabilitation in a different workflow, staffing model, and patient stage.

I always ask departments to start with their therapy pathway. The right device type depends on where the team wants to intervene and how sessions run today.
Overground exoskeletons
An overground gait exoskeleton supports walking practice across the floor, often with a walker or similar support setup. This type gives therapists a more functional walking context. It can fit centers that want mobility-oriented training and flexible use across patient stages.
Treadmill-based systems
These systems usually combine robotic leg guidance with treadmill training, and often with body-weight support. They can work well for highly structured repetitive sessions. They often suit departments that already run treadmill-based neuro rehab workflows.
Hybrid configurations
Hybrid setups combine features from both approaches. A system may support guided overground use and also integrate with other support methods. This model can appeal to departments that treat mixed patient groups and want more than one training format.
| Type | Best fit for | Main advantage | Main trade-off |
|---|---|---|---|
| Overground exoskeleton | Functional gait practice | More natural walking context | Requires careful space and workflow planning |
| Treadmill-based system | High repetition structured sessions | Stable training environment | Less overground transfer feel |
| Hybrid configuration | Mixed rehab pathways | Broader use options | More evaluation needed during purchasing |
For many European buyers, overground systems draw attention because they align with practical ward use and more visible patient engagement. That said, the best answer depends on department goals, not trend value.
What Does a Gait Training Exoskeleton Do for the Therapist?
Therapists often carry the heaviest burden in gait rehab. Manual support work can limit session intensity and create staff fatigue over time.
A powered gait trainer helps therapists reduce manual physical effort and deliver more consistent repetitions. It does not replace therapist skill. It extends what a therapist can do safely and repeatedly during a session.

This point matters more than many product brochures admit. In real hospital settings, staffing pressure shapes equipment value.
Less manual strain
In traditional assisted gait training, one or more therapists may need to support weight shift, limb advancement, trunk control, and safety at the same time. That is physically demanding. A gait training exoskeleton can reduce part of that manual load.
More repetitions per session
Robotic support can help maintain structured stepping for longer periods in selected patients. That may allow more repetition than purely manual handling in some cases. I use careful language here because patient tolerance still sets the limit, and individual results depend on the protocol.
More standardised sessions
A machine can repeat a programmed assistance pattern more consistently than human hands alone. That can help departments build clearer training routines across staff members.
Better commercial fit for distributors and hospitals
When I speak with distributors, I often connect the therapist value to the business case. If a device helps a ward improve workflow and reduce staff burden, the sales discussion becomes more concrete.
Indicative pricing also matters. FOB prices for gait trainers start at approximately €25,000, depending on configuration and volume. Comparable Western brands often sit around €80,000–€100,000 per system. These are indicative ranges only. Exact pricing depends on package, accessories, and order volume. For distributors, the usual margin target is 30–40% when the local market fit is right.
What Does a Gait Training Exoskeleton Not Do?
Exoskeleton marketing can create unrealistic expectations. That creates risk for both clinical adoption and distributor credibility.
A gait training exoskeleton does not cure neurological injury, does not remove the need for therapists, and is not meant for independent home use in standard rehab deployment. It requires patient selection, setup, and clinical supervision.

I believe this is one of the most important parts of the conversation. Honest limits build trust faster than bold claims.
It is not a cure
The device supports gait practice. It does not reverse the underlying condition by itself. Studies have shown feasibility and clinical interest in robotic gait training, but no serious rehab team should present the device as a cure.
It is not independent home walking technology
In the markets we focus on, these systems are used in professional settings. They require assessment, fitting, supervision, and safety procedures.
It is not a shortcut around training quality
A weak protocol stays weak even with advanced hardware. Good outcomes still depend on the therapist, the patient, the progression plan, and the rehab environment.
It is not currently CE marked as a medical device under EU MDR
This point must be clear. GaitExo products are not currently CE marked as medical devices under EU MDR. We act as the trading and branding partner. The importer or distributor is the local responsible party for medical device registration decisions. Our team helps with documentation, export structure, and compliance pathway planning, including HS 8479.89 classification strategy for rehabilitation training equipment. We do not replace the importer’s legal role in the local market.
How Should You Evaluate Fit for Your Department?
A department can become interested in exoskeletons quickly. A good purchasing decision still needs a practical filter.
To evaluate fit, look at patient mix, therapy goals, staffing, space, budget, and compliance pathway. The best gait exoskeleton rehabilitation purchase is the one that matches your real workflow, not the one with the most dramatic demo.

I usually suggest that buyers work through five questions before they ask for a quote.
1. Which patient group will use it first?
Start narrow. Pick one or two clear use cases. Stroke and SCI programs often make the most sense for an initial evaluation because the therapy pathway is easier to define.
2. What does your team want to improve?
Do you want earlier standing practice, more repetitions, less therapist strain, or a stronger advanced rehab offering? One device can support several goals, but one goal should lead the evaluation.
3. Can your workflow support it?
Check staffing, storage, training time, and treatment space. Also check whether your team prefers overground or treadmill-based practice.
4. What is the budget model?
Look beyond purchase price. Include training, accessories, shipping, and launch support. Our standard lead time is 4–8 weeks from order confirmation. We usually work on FOB or CIF terms and provide full English technical documentation, installation guides, and remote support.
5. What is the import and compliance path?
For distributors, this is critical. We help plan export documents, customs workflow, and HS Code 8479.89 strategy. The importer decides the local registration path.
| Evaluation area | Questions to ask |
|---|---|
| Clinical fit | Which patients and goals come first? |
| Workflow | Who sets up, supervises, and stores the system? |
| Budget | What is the full landed and launch cost? |
| Technical support | What training and documents are included? |
| Compliance | Who takes local registration responsibility? |
A rehab distributor in Northern Europe once asked us for a quote on the largest robotic gait system in our range. Their team felt pressure because one hospital customer kept mentioning “advanced robotics,” and everyone assumed the safest move was to show the most complex option first.
Before we sent pricing, we asked one question: “Which patient group will use it in the first three months?”
The room went quiet. After a longer discussion, the distributor admitted the hospital did not have a clear answer. The rehab department treated a mixed caseload. Most patients were stroke cases in transition-phase walking, not early-stage high-support treadmill candidates. The therapy gym was also smaller than expected, and the staff wanted something they could move into normal ward workflow without creating a dedicated robotics room.
That changed the whole project. Instead of quoting the biggest system, we helped them define a narrow first-use scenario: supervised overground gait training for post-stroke patients who could stand and step, but still needed structured walking support. Once that use case became clear, the hospital dropped the idea of a large fixed platform and evaluated an overground solution instead.
The result was simple but important. They avoided buying a system that looked impressive in a presentation but would have seen low daily use. By narrowing the first-use scenario before discussing price, they made a choice that matched their staff, their space, and their real patient flow.
Gait training exoskeletons give rehab teams a structured way to deliver assisted walking practice. Clear definitions, honest limits, and careful fit assessment turn interest into sound decisions.


