

Foot drop is common in neurorehabilitation, but many teams still compare ankle solutions too simply. That leads to poor product matching, unclear expectations, and weak rehab pathway planning.
Passive AFOs and powered ankle assist devices solve different problems. Passive AFOs mainly provide positioning and foot clearance support. Powered ankle exoskeletons add active assistance during gait training. The right choice depends on patient stage, training goal, and whether the device is meant for daily wear or supervised rehabilitation use.

I have seen this category cause confusion for years. A rehab team knows it has many foot drop patients. A distributor sees demand from stroke and neuro clinics. Then everyone starts using the same word, “AFO,” for very different products. That is where decision quality drops. In this article, I will separate the categories clearly and explain where each one fits. If your team wants a more complete lower-limb rehab pathway, this topic matters more than many people think.
What Is Foot Drop and Why Does It Matter in Neurorehabilitation?
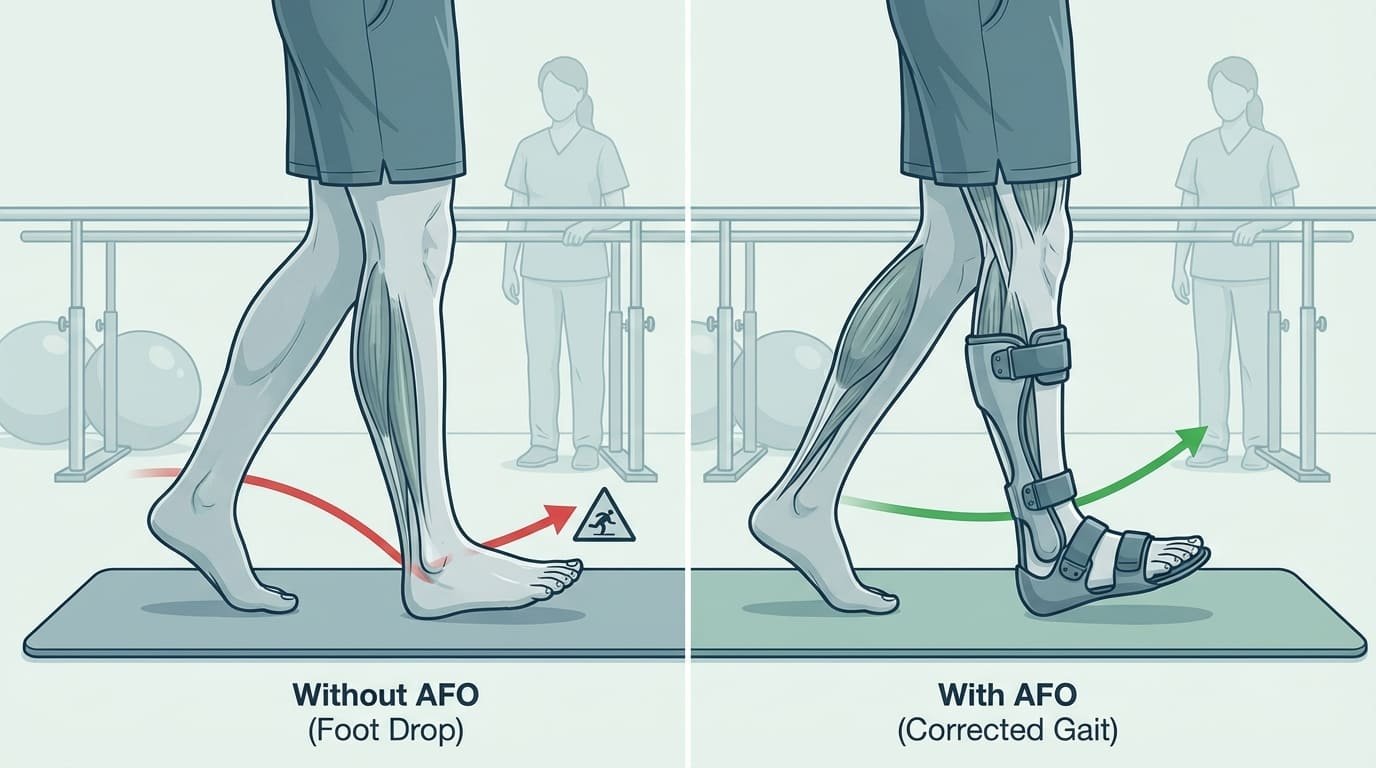
Foot drop sounds like a narrow ankle problem, but in practice it affects walking quality, safety, confidence, and therapy progression across many neuro rehab settings.
Foot drop is a gait problem in which the patient cannot lift the front of the foot well during swing phase. In neurorehabilitation, it often appears after stroke, brain injury, SCI, or other neurological conditions. It matters because poor foot clearance raises fall risk and disrupts step quality.
I think every rehab department understands foot drop clinically. But many purchasing teams still underestimate how often it shapes everyday training decisions. When the foot does not clear well, almost every walking task becomes harder.
Why foot drop changes the whole gait pattern
A patient with foot drop often compensates in other ways. They may hike the hip, circumduct the leg, shorten the step, or walk more slowly. These compensation patterns can make gait training less efficient. They can also increase fatigue and reduce confidence during corridor walking.
Why it matters in hospital rehab
In neurorehabilitation, foot drop affects more than long-term bracing. It affects whether a patient can safely practice walking in the therapy room, in the corridor, and later in more practical settings. This means ankle support decisions influence both immediate rehab work and later mobility planning.
Why the market stays confusing
Many teams still group all ankle devices under one label. But a rigid or passive AFO, a dynamic AFO, and a powered ankle assist device do not serve the same purpose. One focuses on support and positioning. Another may add some flexibility. A powered system adds timed active assistance during gait.
In one clinical meeting, the rehab team opened the discussion by saying, “We need an AFO solution.” At first, everyone in the room seemed to mean the same thing. But after a few questions, we found two very different needs. The ward therapists wanted something that could support gait training sessions and help with active stepping practice under supervision. The orthotics side wanted a simple device for daily wear, long use time, and easy routine management. Once we separated training use from daily wear use, the confusion disappeared. The team realised that a passive or rigid AFO might fit one need, while a powered ankle assist device could fit the other. That changed the conversation from one vague product request into a more useful clinical planning discussion.
The planning takeaway
If a hospital treats stroke or neuro patients at scale, ankle solutions should not be an afterthought. They should be part of a structured lower-limb rehabilitation plan.
Why Do Traditional Passive AFOs Have Limits in Dynamic Gait Training?
Passive AFOs remain useful, but some teams expect them to do more than they are designed to do. That creates disappointment during active gait training.
A traditional passive AFO helps position the ankle and improve foot clearance, but it does not provide powered assistance. In dynamic gait training, its limits often appear when the patient needs active timing, propulsion support, or more natural movement under changing walking conditions.

I want to be fair here. Passive AFOs have an established role. They are familiar, widely used, and often practical. But they are not the answer to every ankle problem in rehab.
What a passive AFO does well
A passive AFO can:
- Help stabilize ankle position
- Improve toe clearance during swing
- Reduce some unsafe movement patterns
- Support daily mobility in many patients
These are meaningful benefits. That is why passive devices remain common in stroke and neuro rehab.
Where the limits appear
In supervised gait training, the therapist may want more than positioning. The therapist may want a device that responds during the gait cycle and supports movement timing. A passive AFO cannot actively generate assistance. It cannot detect gait phase and then push or lift in response.
Why this matters during training
A patient who needs more dynamic ankle support may still show:
- Limited dorsiflexion timing
- Weak step initiation
- Reduced gait smoothness
- Lower tolerance for repeated walking tasks
This does not mean passive AFOs fail. It means they have a defined role.
Daily wear and training are not the same
This point often gets missed. A device that works well for day-to-day support is not always the best tool for active clinical gait training. In many departments, those should be treated as two separate product decisions.
How Do Powered Ankle Assist Devices Work?
Powered ankle devices often interest buyers, but the technology can sound more complex than it really is. The basic idea is simple.
A powered ankle exoskeleton or ankle assist device uses sensors and control logic to detect walking phases and provide active ankle assistance at the right time. In rehab settings, this can support more dynamic gait training than a passive brace alone.

I usually explain this category in one sentence first. A powered ankle device does not just hold the foot. It helps move it.
Gait-phase detection
Many powered ankle systems use sensor input to identify parts of the gait cycle. The system may detect stance and swing timing, then adjust support accordingly. This gait-phase detection is important because the ankle does not need the same help during every moment of walking.
Active assistance
When timed well, the device can assist dorsiflexion or support aspects of ankle movement during training. That can create a more dynamic training feel than a passive support-only brace.
Why this matters in rehab
For selected patients, active assistance may support more repeatable stepping and a more engaging gait training session under professional supervision. Research suggests powered ankle systems are feasible in neurorehabilitation, but individual outcomes depend on patient profile and clinical protocol.
Typical feature areas buyers ask about
| Feature area | Why it matters |
|---|---|
| Gait-phase detection | Determines whether support matches walking timing |
| Assistance mode | Affects how much active support the patient receives |
| Weight and fit | Influences comfort and training tolerance |
| Battery and runtime | Affects session planning |
| Donning time | Impacts therapist workflow |
| Control simplicity | Determines whether the device can be used consistently |
A good powered device should feel clinically usable, not technically impressive but operationally slow.
How Do Powered and Passive Ankle Solutions Compare in Outcomes and Patient Experience?
Teams often ask which one is better. That is the wrong first question because the answer depends on the intended role.
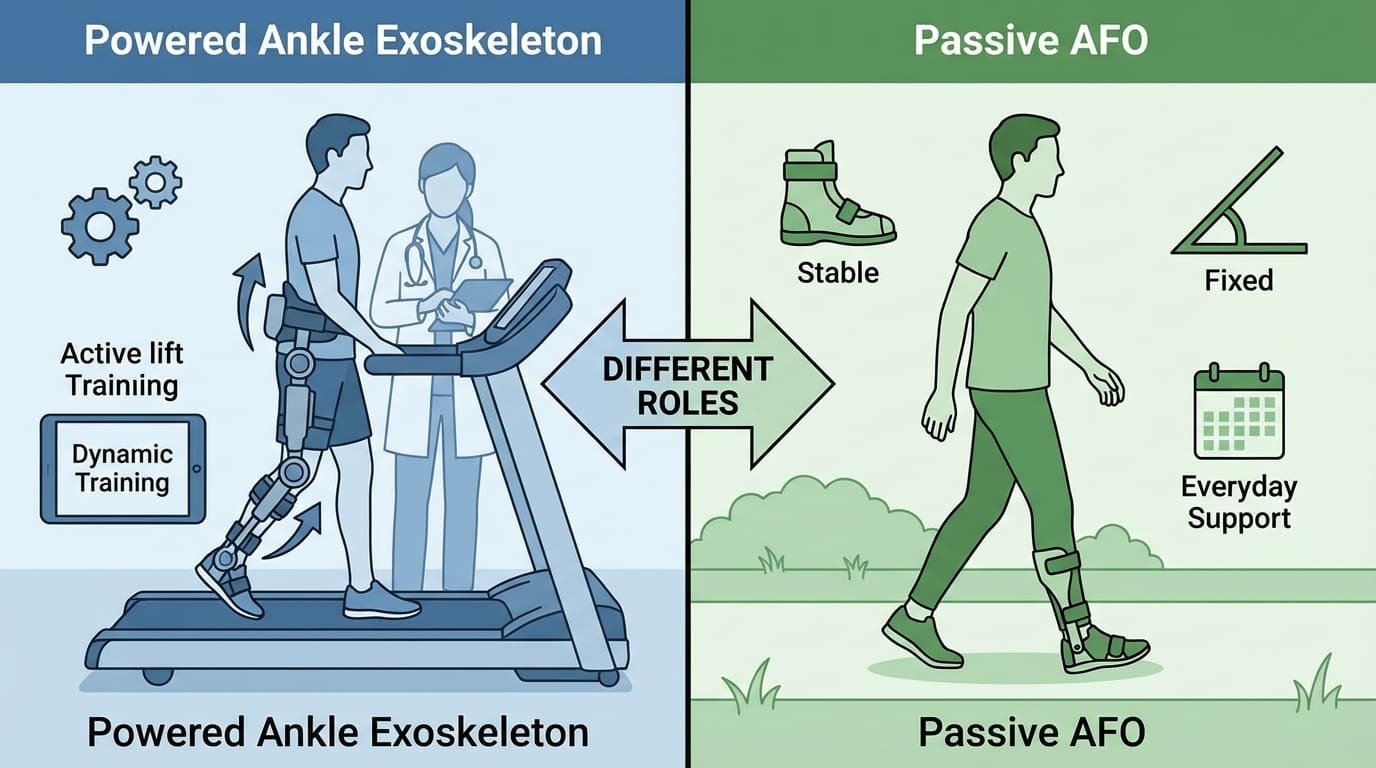
Powered and passive ankle solutions differ in movement support, training potential, and user experience. Passive AFOs often suit everyday support and positioning. Powered ankle assist devices may offer a more dynamic training experience in selected clinical cases under supervision.
I prefer to compare them by purpose, not by hype.
| Comparison area | Passive AFO | Powered ankle assist device |
|---|---|---|
| Main role | Positioning and support | Active gait assistance during training |
| Energy source | None | Powered system |
| Gait response | Fixed or semi-flexible | Sensor-driven timing support |
| Patient feel | Stable and familiar | More active and responsive |
| Daily wear potential | Often stronger | Depends on model and use case |
| Clinical training value | Useful but limited in dynamic assistance | Higher potential for active gait-phase training |
| Complexity | Lower | Higher |
| Cost | Lower in most cases | Higher in most cases |
Clinical outcomes: what we can say honestly
I want to be careful here. We should not over-claim. Research suggests that powered ankle assistance may support gait training feasibility and patient engagement in selected populations. Clinical feedback indicates that some users perceive more natural timing and improved movement confidence. But no device works equally well for every patient, and results depend on diagnosis, severity, protocol, and supervision.
Patient experience matters
Therapists often focus on mechanics, but patient experience also matters. Some patients value simplicity and stability. Others respond better to a more active assisted feel. This is one reason a trial period can be useful before larger rollout.
Which Patients Benefit Most From Powered Ankle Assist?
Powered ankle support sounds attractive, but it is not the right answer for every foot drop case. Good patient selection matters.
Patients who may benefit most from powered ankle assist include selected stroke patients, neuro rehab patients in active gait training, and users who need more dynamic assistance than a passive AFO can provide. Selection depends on cognition, walking tolerance, ankle deficit pattern, and training goals.

I usually suggest that hospitals think in terms of “training candidates” rather than “all foot drop patients.”
Common strong-fit profiles
- Stroke patients in supervised gait training
- Neuro patients with persistent dorsiflexion weakness
- Patients progressing from heavier gait support toward more active walking
- Cases where passive support improved safety but did not fully support dynamic training goals
Cases that need caution
Some patients may still be better served by a passive solution because they need simplicity, lower complexity, or long daily wear rather than active training support.
Screening questions
| Selection question | Why it matters |
|---|---|
| Is the patient in active gait rehabilitation? | Powered assist is often more valuable during training |
| Does the patient need timed ankle help, not only positioning? | Clarifies if active assistance is relevant |
| Can the patient tolerate the device and follow cues? | Supports safe supervised use |
| Is the rehab goal dynamic gait improvement? | Aligns technology with therapy purpose |
I remember a stroke case that showed this difference very clearly. The patient first used a passive support solution because the team needed something simple, safe, and easy to tolerate during early walking practice. That choice made sense at the time, and it helped with positioning and basic stability. But during later supervised training sessions, the therapists noticed that the patient responded better when active ankle assistance was introduced. The stepping pattern became more purposeful, and the patient engaged more with the training task. The passive option still had value for simple support, but the active device gave the team a different tool when the rehab goal shifted toward dynamic gait practice. That case reminded everyone that safety, tolerance, and training purpose all matter when choosing between passive and powered support.
Why Should Rehab Teams Separate Daily Use AFOs From Clinical Training AFOs?
This is one of the most important distinctions in the whole category, and many teams still blur it.
A daily use AFO and a clinical training AFO often serve different purposes. Daily use devices prioritize practicality, wearability, and routine mobility support. Clinical training ankle devices prioritize supervised gait practice, movement quality, and therapy-specific progression.

I think this single distinction can improve many purchasing discussions. Once a department accepts that these are different jobs, the product map becomes much clearer.
Daily use AFO
A daily use AFO usually aims to support routine mobility through the day. It needs to be practical, acceptable for repeated wear, and easy to manage.
Clinical training AFO or powered ankle assist
A clinical training device may be used during rehab sessions under therapist supervision. The goal is not just to support walking safely. The goal is to shape training quality.
Why one device may not do both well
The best daily brace is not always the best dynamic rehab tool. The best powered training device is not always the simplest all-day mobility aid.
| Product role | Priority |
|---|---|
| Daily use AFO | Simplicity, support, wear time |
| Clinical training AFO | Therapy goals, gait quality, supervised use |
| Powered ankle assist | Active dynamic assistance, gait-phase timing |
This distinction also helps distributors. Instead of trying to sell one universal answer, they can present a clearer pathway-based solution.
How Do Ankle Solutions Complete the Lower-Limb Rehabilitation Pathway?
Ankle devices often look small beside large robotic gait systems, but they complete the pathway in a very practical way.
Ankle solutions complete the lower-limb rehabilitation pathway by addressing foot clearance and ankle control during the stages between intensive gait training, transition walking, and longer-term mobility support. They connect high-level robotic rehab with practical walking function.

I see this clearly when we discuss full department planning. A hospital may invest in a Gait Training Exoskeleton for intensive robotic work. It may also explore a Hip Assist Exoskeleton for transition-phase walking. But if the patient still has unresolved foot drop, the pathway remains incomplete.
A simple pathway view
| Rehab stage | Main need | Device category |
|---|---|---|
| Intensive gait restoration | Structured walking practice | Gait Training Exoskeleton |
| Transition walking progression | Mobile walking assistance | Hip Assist Exoskeleton |
| Distal gait control and foot clearance | Ankle support and gait refinement | Ankle Assist & AFO Solutions |
Why this matters for hospitals
A complete portfolio helps the department treat more of the actual walking problem, not only the most visible part of it. That is also why many buyers now prefer pathway planning over single-device purchasing.
Why this matters for distributors
A broader lower-limb product strategy gives distributors more ways to fit real hospital needs. It also creates a more stable commercial model than relying on one flagship product.
At GaitExo, we focus on this full pathway logic across Gait Training Exoskeleton, Hip Assist Exoskeleton, and Ankle Assist & AFO Solutions. We act as the trading and branding partner, not the manufacturer. Our manufacturing partners include EULON (优龙机器人). We provide English technical documentation, export support, and practical planning for distributors and hospitals. Standard lead time is 4–8 weeks from order confirmation. We usually work on FOB or CIF terms.
I also need to state the compliance boundary clearly. GaitExo products are not currently CE marked as medical devices under EU MDR. The importer or distributor remains the local responsible party for medical device registration decisions. We can support documentation and HS 8479.89 planning where relevant, but local regulatory responsibility stays with the importer.
Foot drop needs clearer device selection, not broader marketing claims. When teams separate passive support from powered training roles, ankle solutions become much easier to evaluate.


